

Reform Psychiatry – Informed Consent, Black Box Warnings and Genetic Testing
Reform Psychiatry – Informed Consent, Black Box Warnings and Genetic Testing
The Issue
To: U.S. Congress, FDA, American Psychiatric Association, and Mental Health Providers Nationwide
We, the undersigned, call for an immediate reevaluation of psychiatric drug prescribing practices. This includes:
▶Transparent, mandatory disclosure of Black Box warnings
▶Routine offering of pharmacogenetic testing (e.g., GeneSight)
▶Informed consent policies that fully educate patients—especially youth—on potential risks
▶Greater emphasis on alternatives to medication-first approaches in mental health care
My Story: A Cautionary Tale of Blind Trust in the System
At just 16, I was forcibly placed on psychiatric medications including Lexapro, Wellbutrin, Adderall, and later Klonopin. I trusted the professionals who said it was the best path forward for my specific issues that only snowballed the more time I spent in their care. But instead of feeling better, I spiraled into unfamiliar emotional states, losing touch with my inner compass. It wasn’t until 2019, when I stopped taking them entirely and transitioned to PRNs and a different type of protocol only, that I truly started to recover. With some expected hiccups due to a recent head injury.
I’m not here to vilify doctors. They did what they believed was right with the education they had. But I believe there's a bigger truth being ignored: psychiatric medications are not for everyone, and in my case, they caused more harm than good. I later found out through a gene sight test that many of the drugs my therapist said "she would stop seeing me for if I didn't take" I was actually highly allergic to and was taking for years!!!
The sad truth? Sometimes you’re prescribed a drug for depression or lack of focus, only to become so wired that you then need medication for anxiety. Over time, you lose touch with your natural rhythms—feeling both wired and exhausted—and need an “off/on switch via a pill” just to function. When that switch stops working, doctors often add new layers of medication to “top you off” and treat the symptoms caused by previous drugs.
Mix that with occasional alcohol or cannabis use, and over time you’re creating a recipe for a potential psychotic breakdown. What late teen or young adult struggling with depression doesn’t sometimes use these substances—whether it’s “hanging out with friends” or trying to appear “normal,” even while knowing deep down that mixing recreational drugs with prescribed medications can lead to irreversible consequences? Some of these consequences are so serious they can even lead to arrest. Many people don’t realize why their personality or behavior has changed. It’s incredibly difficult to be fully self-aware of these shifts—especially if you’re isolated or simply living through the experience. Expecting someone who is unwell, injured and cycling in and out of episodes to step back and objectively observe themselves isn’t fair. Asking them to have insight into their condition while they are still in the midst of it—and then holding them accountable for that lack of insight—raises serious ethical concerns.
This is how severe the risks are. When these behavioral changes happen, people often blame it solely on the recreational substances—“It’s the pot,” they say—but rarely do they consider the role of the prescribed pills. The medication’s impact is too often overlooked. If you speak out about these issues, you’re often dismissed as a conspiracy theorist or accused of being anti-science...a bad influence. People who swear by their medications sometimes tell you to stay quiet because the drugs “saved their life.” And that’s great—if it worked for you, I’m truly glad. But it didn’t work for me, and my experience deserves to be heard—because there are others out there who feel too isolated or afraid to speak up against the mainstream expectations around medication and mental health. Too often, the moment someone “appears not to be doing well,” the first question asked is, “Are you taking your meds?” as if nothing else could possibly be causing their struggles.
For starters, let’s consider the economic fallout of long-term mental health challenges—and the soul-crushing weight of realizing that your life’s trajectory has shifted dramatically from what your younger self once expected. As a teen, everyone assumed you’d do well in life, but after years of taking psychiatric medications, your adult reality feels far from that hope. It’s like the classic chicken-or-egg question: did the reckless behavior come from taking drugs that caused excessive energy—like Adderall or Wellbutrin—or was it the weekend beers and cannabis? Why is it that you never craved cannabis or alcohol until you started those excitatory medications? And how did Lexapro dull your emotions so much that you felt you needed those substances just to have a conversation, instead of feeling like a blank mute?
One can’t help but wonder if many of the choices or life decisions made would have been more in alignment with who someone was before all of this mental health intervention and analysis, rather than after. The person I was before would have been far more careful, while the person I became afterward was much more reckless.
Not much thought is given—or at least not explained in layman’s terms—about the long-term impacts of starting these drugs early, just as the brain’s scaffolding and prefrontal cortex are still developing and strengthening. It makes sense, then, that questioning these treatments isn’t crazy or ludicrous. No one explains what happens if you stop taking a drug you’ve been primed to rely on—even after realizing it wasn’t good for you. Maybe it’s because they don’t have clear official guidance on how to manage that process yet.
Most therapists or experts will say, “These drugs are proven to HELP, and they can REVERSE the effects of depression, which we KNOW you have based on this 5-minute questionnaire.” That diagnosis can then define your whole identity for life and pressure you into believing how crucial the medication is—forever. But it’s also important to remember that this framing is part of their job.
Is it fair to blame all of this solely on the meds or the mental health system? Certainly not—it’s a complex, multifaceted issue. But it’s absolutely reasonable to recognize medication mismanagement and physiological incompatibility as a significant contributing factor in that difficult journey.
What’s a boon for someone else can be a bane for you.
The increase in prescribing antipsychotics over the past 7–10 years has led to a rise in side effects like tremors—symptoms that once were less common. Some treatment centers even resort to ECT (electroconvulsive therapy), despite repeated evidence of serious, long-lasting side effects.
What Are Black Box Warnings?
▶Black Box Warnings are the FDA’s most serious alert for prescription drugs, highlighting risks of serious, life-threatening adverse effects, such as:
▶Suicidal ideation (especially in teens and young adults)
▶Increased aggression
▶Severe withdrawal symptoms
▶Long-term neurological impacts
▶SSRIs (like Prozac), SNRIs, benzodiazepines, and antipsychotics often carry such warnings—but these are rarely explained properly to patients.
Emotional numbing and reduced empathy can be side effects associated with some psychotropic medications, including those with black box warnings. Here's how:
▶Emotional numbing (or emotional blunting) is commonly reported with many antidepressants, especially SSRIs like fluoxetine (Prozac), sertraline (Zoloft), and escitalopram (Lexapro).
▶Patients often describe feeling less able to experience a full range of emotions—both positive and negative—which can feel like a “flattening” or “numbing” effect.
▶Reduced empathy is less commonly discussed but has been reported anecdotally and in some studies. Some people on certain antidepressants or antipsychotics report feeling more detached from others emotionally, which can impact social relationships.
▶Antipsychotics may also contribute to emotional blunting or diminished affect as part of their sedative and dopamine-blocking effects.
▶These effects are not universal, but they are recognized enough to be concerns discussed in psychiatric and patient communities.
Sources in a numbered list for easy reference:
▶University of Cambridge study on emotional blunting caused by antidepressants
https://www.cam.ac.uk/research/news/scientists-explain-emotional-blunting-caused-by-common-antidepressants
▶Psychiatrist.com article on why antidepressants cause emotional blunting
https://www.psychiatrist.com/news/why-antidepressants-cause-emotional-blunting/
▶Study on antidepressants reducing pain empathy (Translational Psychiatry)
https://pubmed.ncbi.nlm.nih.gov/31175273/
▶Qualitative study on emotional blunting from long-term antipsychotic use
https://journals.kmanpub.com/index.php/prien/article/view/3341
▶British mental health charity Mind on antipsychotics and side effects
https://www.mind.org.uk/information-support/drugs-and-treatments/antipsychotics/side-effects/
Furthermore, many psychotropic medications—especially certain antipsychotics and some mood stabilizers—are linked to serious physical health risks such as metabolic syndrome, which includes weight gain, diabetes, high blood pressure, and increased risk of heart disease. These side effects can drastically affect overall health and quality of life, yet they are often downplayed or not fully explained to patients before starting treatment.
The most serious concern of all is the risk of suicidal ideation and aggressive behavior, particularly among adolescents and young adults. The FDA has issued black box warnings for certain antidepressants, indicating an increased risk of suicidal thoughts and behaviors in this age group.
While some studies have investigated potential links between psychiatric medications and violent incidents, such as school shootings, the findings are complex and not definitive. For instance, a study published in Behavioral Sciences & the Law found that most school shooters were not previously treated with psychotropic medications, and no direct or causal association was established.
However, individual cases have raised concerns. For example, Eric Harris, one of the perpetrators of the Columbine High School massacre, was prescribed fluvoxamine (Luvox), an SSRI antidepressant. Additionally, the shooter in the 2008 Northern Illinois University incident had been prescribed Prozac, Xanax, and Ambien, and reportedly stopped taking Prozac shortly before the event.
These instances underscore the importance of careful monitoring and informed decision-making when prescribing psychotropic medications, especially to young individuals. It's crucial to balance the benefits of treatment with the potential risks, ensuring that patients and their families are fully informed.
Starting or stopping psychiatric medications suddenly can cause serious, even dangerous, side effects. Here’s why, especially when it comes to things like aggression, violence, or even death:
1. Brain Chemistry Disruption
▶Psych meds (like antidepressants, antipsychotics, mood stabilizers, benzodiazepines, stimulants, etc.) work by altering neurotransmitters—like serotonin, dopamine, norepinephrine, and GABA. These chemicals regulate mood, impulse control, anxiety, and more.
▶When you stop suddenly, the brain is thrown into chemical chaos. It has adjusted to the medication and needs time to recalibrate. Without that transition, things can go very wrong—fast.
2. Withdrawal vs. Relapse vs. Rebound Effects
▶Withdrawal: Your brain struggles without the drug it's used to, sometimes mimicking or worsening the symptoms it was treating.
▶Relapse: The original condition may come back stronger.
▶Rebound: Some symptoms (like anxiety or insomnia) can come back even worse than before—often temporarily—but severely.
This can lead to:
▶Severe irritability or rage
▶Impulsivity or agitation
▶Paranoia or panic
▶Suicidal or homicidal thoughts in extreme cases
3. Benzodiazepines and Antidepressants Are Particularly Risky
▶Benzodiazepines (e.g., Xanax, Ativan): Stopping suddenly can cause seizures, psychosis, or extreme aggression.
▶SSRIs/SNRIs (e.g., Zoloft, Effexor): Can cause “SSRI discontinuation syndrome” — brain zaps, depersonalization, mood swings, etc.
▶Antipsychotics: Sudden withdrawal can cause rebound psychosis or mania.
4. Every Brain Is Different
Some people might feel just a little weird, others might feel like they’re losing control or becoming a different person. Underlying mental health conditions can be exacerbated, like a head injury/post concussive syndrome/TBI (Traumatic Brain Injury), and emotional regulation can become seriously impaired.
5. Why It Can Turn Violent
▶The frontal lobe (responsible for decision-making and impulse control) is often already compromised in psychiatric conditions.
▶Rapid withdrawal or incorrect dosing can impair it further.
▶That’s why stories of sudden violence (including self-harm or harm to others) are linked in rare—but real—cases of abrupt medication changes.
▶The frontal lobe—especially the prefrontal cortex—is deeply involved in many psychiatric conditions. It plays a key role in decision-making, emotional regulation, impulse control, motivation, and social behavior. When psychiatric conditions affect this region, it can lead to many of the symptoms we associate with mental illness.
Here’s a breakdown:
🧠 What Does the Frontal Lobe Do?
▶Executive function: planning, organizing, prioritizing
▶Impulse control: stopping inappropriate behaviors
▶Emotional regulation: managing mood and reacting appropriately
▶Social behavior: empathy, moral reasoning, understanding consequences
▶Attention and focus
▶Motivation and initiative
🔥 How It’s Affected in Psychiatric Conditions
1. Depression
Underactivity in the dorsolateral prefrontal cortex
This leads to:
▶Poor concentration and planning
▶Lack of motivation
▶Difficulty making decisions
▶Emotional flatness or excessive guilt
2. ADHD
Impaired function of the prefrontal cortex
Leads to:
▶Impulsivity
▶Poor attention
▶Difficulty with delayed gratification
3. Bipolar Disorder
During mania: frontal lobe activity decreases, leading to:
▶Poor judgment
▶Risk-taking behavior
▶Grandiosity
▶During depression: similar to MDD, with hypoactivity in frontal circuits
4. Schizophrenia
Hypofrontality—reduced blood flow and activity in the frontal lobe
Causes:
▶Disorganized thinking
▶Poor insight
▶Impaired executive function
▶Emotional blunting
5. PTSD
▶Disrupted communication between the prefrontal cortex and amygdala
▶The amygdala becomes hyperactive (fear), while the frontal lobe fails to properly inhibit it
Result: heightened emotional reactivity and poor regulation
6. Substance Use Disorders
Chronic use of drugs (especially stimulants, alcohol, or opioids) impairs frontal lobe function
Leads to:
▶Impaired judgment
▶Impulsivity
▶Craving cycles and relapse behavior
🧪 Brain Imaging Evidence
Technologies like fMRI and SPECT scans (which Amen Clinics uses) show that people with psychiatric disorders often have:
▶Decreased blood flow to frontal regions
▶Reduced gray matter volume
▶Disrupted connectivity between frontal areas and emotional centers like the limbic system
🔄 Why This Matters for Behavior
When the frontal lobe is compromised, a person may:
▶Struggle to regulate emotions (e.g., sudden outbursts)
▶Make poor or risky decisions
▶Act impulsively without considering consequences
▶Feel “flat” or overly reactive
▶This is one reason why med changes, trauma, or stress can push someone into a dangerous state—they're already operating with reduced “brakes,” and when emotional “gas pedals” like the amygdala kick in, it can overwhelm their ability to self-regulate.
What to Do:
▶Never stop psychiatric meds cold turkey without medical supervision.
▶Taper slowly under a doctor’s guidance.
▶Report any sudden mood changes immediately.
💥 Why Starting or Stopping Psych Meds Suddenly Can Lead to Violence, Rage, or Even Death
It sounds extreme, but sudden changes in psychiatric medication — especially stopping "cold turkey" — can absolutely lead to severe side effects like aggression, violence, psychosis, and in rare cases, suicide or death. One of the most alarming contributors to this is a condition called akathisia.
🧠 The Brain on Psych Meds
Psych medications affect neurotransmitters—chemicals that control mood, energy, anxiety, impulse control, sleep, and more. Over time, your brain adjusts to the presence of these drugs.
Suddenly removing or drastically altering them doesn’t give the brain time to adapt. The result? A chaotic chemical imbalance that can lead to:
▶Extreme agitation
▶Mood swings
▶Paranoia
▶Impulse control loss
▶Intense restlessness or anxiety
🚨 What Is Akathisia?
Akathisia is a movement and mental restlessness disorder often caused by starting, stopping, or changing the dose of antipsychotics, SSRIs, or other psych drugs.
Symptoms:
▶A feeling of being trapped inside your own skin
▶Compulsive pacing, rocking, or leg movement
▶Intense internal torment
▶Inability to sit still
▶Rage or suicidal thoughts driven by mental agony
▶People with akathisia often feel like they're going insane. They may appear agitated or hostile. Tragically, many cases of sudden suicide or violence following medication changes have been linked to undiagnosed akathisia.
📉 Withdrawal, Rebound, and Relapse
When people stop psych meds suddenly:
▶Withdrawal kicks in (shakes, insomnia, anxiety, confusion).
▶Rebound symptoms can be worse than the original condition (e.g., panic, depression, mania).
▶Relapse of the underlying illness can occur fast—and more severely.
▶Combined, this creates a perfect storm for dangerous behavior, especially if akathisia is part of the picture.
⚠️ Real-World Examples
▶SSRIs (like Paxil or Zoloft): Discontinuation can cause akathisia, panic attacks, electric shock sensations, and aggression.
▶Antipsychotics (like Abilify or Risperdal): Sudden withdrawal can lead to psychosis, akathisia, or even catatonia.
▶Benzodiazepines (like Xanax or Klonopin): Cold-turkey withdrawal can cause seizures, psychotic breaks, and violent outbursts.
✅ What to Do Instead
▶Always taper slowly under medical supervision—especially with meds like SSRIs, SNRIs, antipsychotics, and benzos.
▶Watch for signs of akathisia—especially after dose changes.
▶Be honest with your doctor about side effects—agitation is not just “anxiety.”
▶If you or someone else feels “not in control” after a med change, get help immediately. Time matters.
⚠️ Why Gabapentin and Stimulants (like Adderall) Can Be Dangerous
🔹 Gabapentin (Neurontin)
Originally approved for seizures, gabapentin is now commonly prescribed off-label for anxiety, insomnia, pain, and more. But it’s not without risk:
🚨 Dangers of Gabapentin:
▶Sedation + respiratory depression when combined with opioids, benzos, or alcohol (can be fatal)
▶Withdrawal effects: stopping suddenly can cause anxiety, agitation, insomnia, tremors—even seizures
▶Mood instability: some report increased suicidal thoughts, hostility, or mania (especially with bipolar)
▶Dependence: despite not being a controlled substance everywhere, it’s increasingly abused for its calming or euphoric effects
▶Cognitive dulling: can cause "brain fog," slowness, or affect memory
🧠 Frontal Lobe Impact:
▶Can dampen excitatory brain activity, leading to emotional flattening, impulsivity, or disinhibition in some
▶May interfere with mood regulation, especially if taken long-term or in high doses
🔹 Stimulants (e.g., Adderall, Ritalin, Vyvanse)
▶These are amphetamines or methylphenidate-based meds used for ADHD. When carefully prescribed, they can improve focus and impulse control. But they carry serious risks, especially when:
▶Overused
▶Mixed with other drugs
▶Taken without ADHD
▶Stopped abruptly
🚨 Dangers of Stimulants:
▶Increased heart rate and blood pressure — raises risk for stroke, arrhythmias, even sudden death in vulnerable individuals
▶Anxiety, panic, or paranoia (especially at high doses or when sleep-deprived)
▶Mania or psychosis in people with bipolar or schizophrenia
▶Aggression and impulsivity — overstimulation of the brain’s “go” systems can override normal self-control
▶Crash and rebound depression when the drug wears off or is suddenly stopped
▶Addiction risk: Adderall is a Schedule II controlled substance for a reason — tolerance builds, and misuse can spiral quickly.
🧠 Frontal Lobe Impact:
Stimulants intensify dopamine and norepinephrine in the prefrontal cortex — which improves focus short-term but can:
▶Overload emotional regulation
▶Trigger rage, obsessive behavior, or paranoia
▶Impair long-term balance in brain reward circuits
❗When Combined (or Used Without a Clear Diagnosis)
Using gabapentin + stimulants, or either one in someone with undiagnosed bipolar, trauma, or psychotic risk, can be a recipe for disaster:
▶May cause emotional instability, outbursts, panic, or aggression
▶Masks symptoms instead of addressing the root cause
▶May be seen as “safe” — leading to under-monitoring and dangerous self-medication or withdrawal
🔄 Key Rule: Start low, go slow, taper gently, and monitor carefully.
Just because a drug is common doesn't mean it's harmless. Your brain is a finely tuned system — even small shifts in neurotransmitters can dramatically change behavior, perception, and mood.
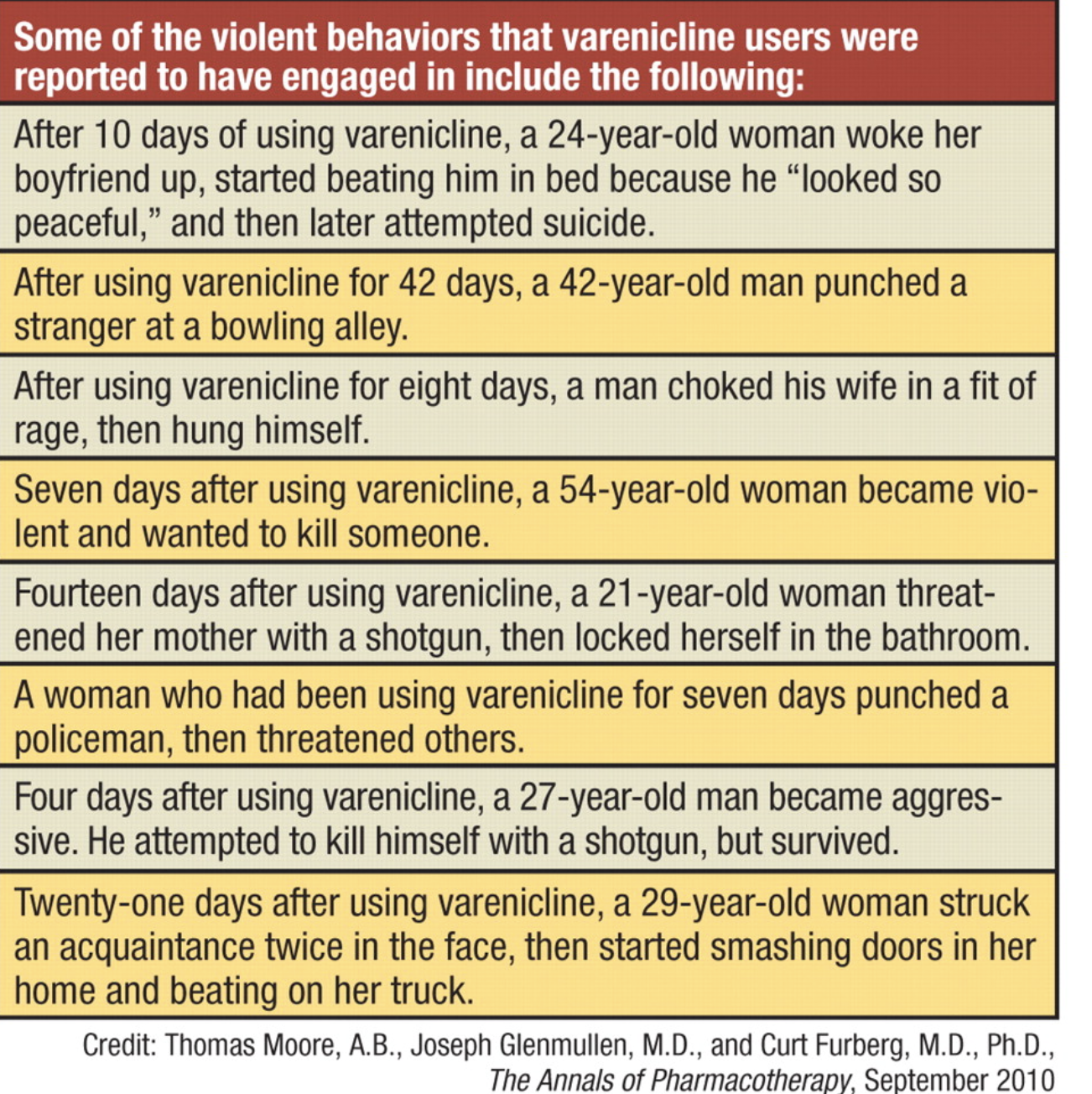
Varenicline (Chantix) and bupropion (Wellbutrin, also called Budeprion) are essentially the same chemical compound. There is a significant difference between Wellbutrin XL (extended-release) and Wellbutrin SR (short-release). About seven years ago, there was a recall involving this medication. Both starting and abruptly stopping Wellbutrin can increase the risk of seizures.
What’s interesting is that this is a clear example of rebranding and off-label use—where the same substance is packaged and promoted for entirely different purposes. For example, bupropion was originally developed as an antidepressant (Wellbutrin), but later rebranded for smoking cessation (Chantix). Similarly, Vyvanse, a stimulant approved for ADHD, was also marketed for binge eating disorder—despite the fact that it can be particularly risky or easily abused by individuals with a history of eating disorders.
- Fluoxetine (Prozac) and Workplace Violence
In 1989, Joseph T. Wesbecker killed eight people and injured twelve before committing suicide. He had begun taking fluoxetine (Prozac) 11 days prior. His relatives and victims attributed his actions to the medication, leading to a lawsuit against the manufacturer, Eli Lilly, which settled for $50 million across 300 claims. Internal documents revealed that fluoxetine had been linked to suicide attempts during clinical trials, raising concerns about its safety.
2. Maharishi University of Management Stabbing
In 2004, a student at Maharishi University of Management in Iowa fatally stabbed a fellow student. The perpetrator, diagnosed with schizophrenia, had been off his medication for months at the time of the incident. He was later found not guilty by reason of insanity, highlighting the potential risks of discontinuing psychiatric medication.
3. Antidepressant-Induced Violence
Studies have shown that certain antidepressants, such as venlafaxine (Effexor) and fluvoxamine (Luvox), are more likely to be associated with violent behavior compared to other drugs. For instance, venlafaxine is 8.3 times more likely to be linked with violence than other medications .
4. Benzodiazepine Abuse and Aggression
Flunitrazepam, a benzodiazepine, has been implicated in cases of extreme aggression and violence. Forensic psychiatric patients who abused flunitrazepam exhibited violent behavior, lack of empathy, and impaired judgment, often in combination with alcohol or other drugs .
5. 25I-NBOMe and Hallucinogenic-Induced Violence
25I-NBOMe, a synthetic hallucinogen, has been linked to several violent incidents. In 2015, a 20-year-old student in California died after consuming 25I-NBOMe and engaging in a violent episode. In the UK, a teenager fatally stabbed his friend during a psychotic episode induced by the drug .
(I’ve gone back to my old pharmacy and obtained all records from when I first started taking medications—going back as far as possible—and I’ve been prescribed nearly all of these drugs except five and two. That tells me a lot, including how early and easily doctors, who clearly just saw me as someone to get in and out of their office, were willing to prescribe serious medications without knowing anything meaningful about who I was or the impact of these drugs on my life)
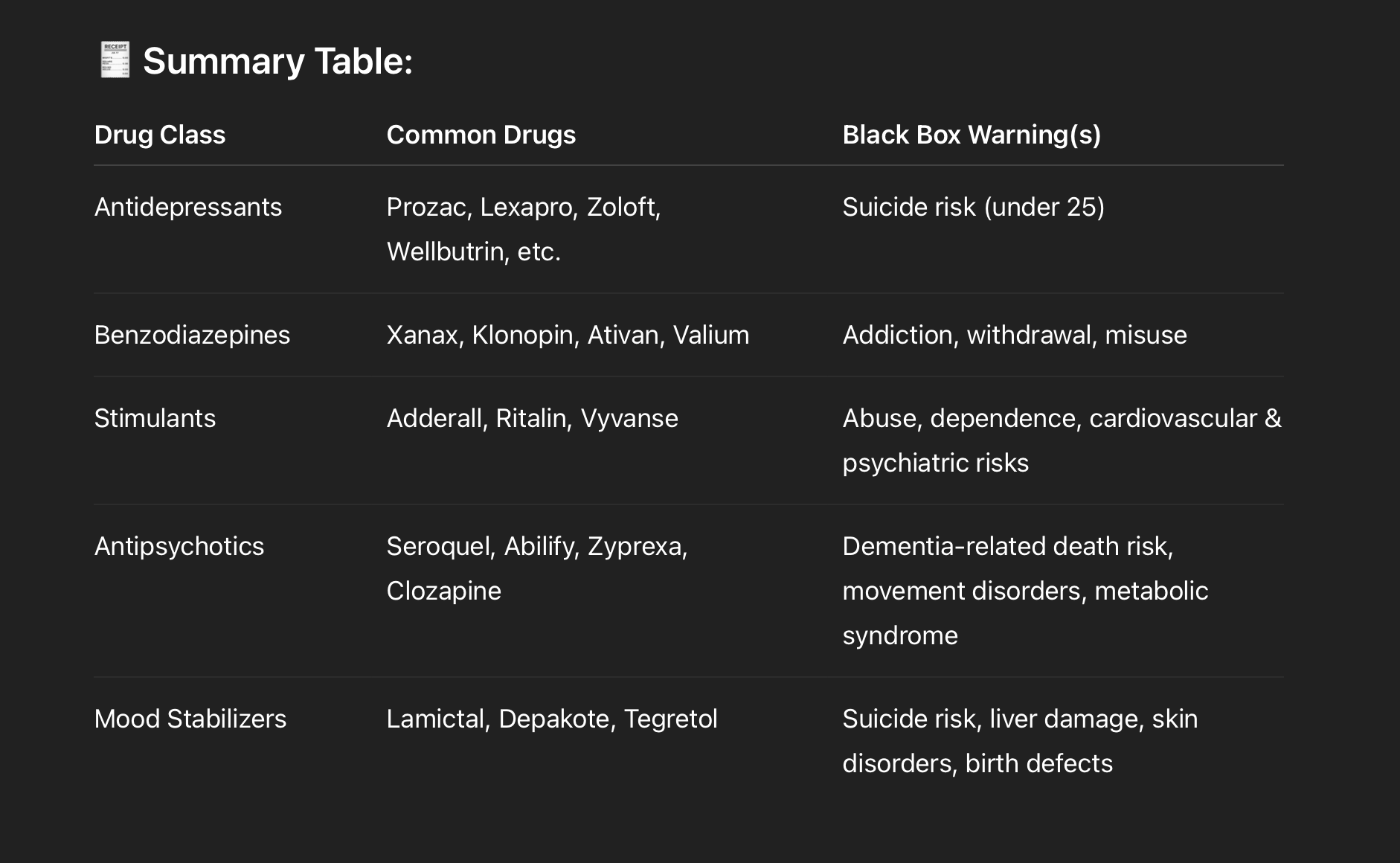
Here's a list of common psychiatric and mental health medications that carry FDA Black Box Warnings—the strongest warning the FDA issues. These warnings highlight serious or life-threatening risks such as suicidal ideation, addiction, withdrawal, respiratory depression, or irreversible side effects.
⚠️ BLACK BOX WARNED PSYCHIATRIC DRUGS:
🧠 Antidepressants (SSRIs, SNRIs, TCAs, MAOIs)
All antidepressants approved for depression carry a Black Box Warning for:
▶Increased risk of suicidal thinking and behavior in children, adolescents, and young adults (up to age 24).
Examples:
▶Fluoxetine (Prozac)
▶Sertraline (Zoloft)
▶Citalopram (Celexa)
▶Escitalopram (Lexapro)
▶Paroxetine (Paxil)
▶Venlafaxine (Effexor)
▶Duloxetine (Cymbalta)
▶Desvenlafaxine (Pristiq)
▶Amitriptyline (Elavil)
▶Nortriptyline (Pamelor)
▶Bupropion (Wellbutrin) – Also carries seizure risk warning.
💊 Benzodiazepines (Anti-anxiety, Sedative)
In 2020, the FDA added a Black Box Warning to all benzodiazepines:
Serious risks of abuse, misuse, addiction, physical dependence, and withdrawal reactions—even when used as prescribed.
Examples:
▶Alprazolam (Xanax)
▶Clonazepam (Klonopin)
▶Lorazepam (Ativan)
▶Diazepam (Valium)
▶Temazepam (Restoril)
⚡ Stimulants (ADHD medications)
Many stimulants used to treat ADHD carry Black Box Warnings for:
▶High potential for abuse and dependence; sudden cardiac death or serious cardiovascular events; psychiatric adverse events (mania, aggression, psychosis).
Examples:
▶Adderall (amphetamine/dextroamphetamine)
▶Ritalin (methylphenidate)
▶Concerta (methylphenidate ER)
▶Vyvanse (lisdexamfetamine)
▶Dexedrine (dextroamphetamine)
🧩 Antipsychotics (Typical & Atypical)
Most antipsychotics carry Black Box Warnings for:
▶Increased mortality in elderly patients with dementia-related psychosis.
▶Some also warn of metabolic side effects, movement disorders (e.g., tardive dyskinesia), and neuroleptic malignant syndrome.
Examples:
▶Risperidone (Risperdal)
▶Olanzapine (Zyprexa)
▶Quetiapine (Seroquel)
▶Aripiprazole (Abilify)
▶Ziprasidone (Geodon)
▶Haloperidol (Haldol)
▶Lurasidone (Latuda)
▶Clozapine (Clozaril) – Also has a unique black box warning for agranulocytosis (fatal blood disorder), seizures, and myocarditis.
🧬 Mood Stabilizers & Anticonvulsants (often used for Bipolar Disorder)
Some mood stabilizers and anticonvulsants have Black Box Warnings for:
Suicidal behavior and ideation and life-threatening skin reactions (like Stevens-Johnson syndrome).
Examples:
▶Lamotrigine (Lamictal)
▶Valproic acid / Divalproex (Depakote) – also has warning for hepatotoxicity, teratogenicity, pancreatitis
▶Carbamazepine (Tegretol)
▶Oxcarbazepine (Trileptal) – similar risks
When the System Fails the Vulnerable
There are haunting real-world consequences when risks are ignored. One such case is that of a woman in Virginia who, just days after being prescribed Prozac, took her own life and the lives of her children. These tragic outcomes are too often brushed under the rug by pharmaceutical companies and professional boards like the APA.
Documentaries like “Psychiatry: An Industry of Death” highlight the historical and ongoing collusion between pharma and psychiatry, raising red flags about overdiagnosis, overmedication, and profit-driven treatment models. This documentary is highly controversial and has faced significant public backlash—first, due to its association with Scientology propaganda, and second, because many believe it promotes harmful views that undermine modern, evidence-based mental health care. However, having watched it twice, I found that it presents an alternative perspective on mental health—one that, while unsettling, offers insight into its historical roots and raises important questions that are often overlooked.
Source: https://www.cchr.org/quick-facts/introduction.html
Why Aren’t We Using Tools Like GeneSight?
Pharmacogenetic testing has been available since 2011. These tests analyze how your unique DNA may influence your response to medications—helping avoid dangerous side effects. Yet, most mental health providers never mention it, especially in insurance-based clinics.
Wouldn’t you want to know which drugs your body is genetically incompatible with before putting them in your system?
The Bigger Picture: A Chemical Trap
Mental health is not one-size-fits-all. Yet the industry often treats psych drugs as the only viable solution. Antipsychotics, for instance, are increasingly prescribed—even off-label—despite severe risks like metabolic syndrome, tardive dyskinesia, and lifelong dependency. Patients are rarely warned about these outcomes.
Many are discouraged from questioning their prescriptions. I remember being told things when I was in my early twenties like, “Oh stop, you’re too pretty to be sad just smile!,” or “You just need a chemical fix.” But my struggles weren’t superficial—they were deeply personal and increasingly chemical, because of the drugs themselves.
Oftentimes, patients are told that the risk of serious side effects is clinically marginal—that statistically, it "would never be you." Well, guess what? It was me. And honestly, I’m still kind of annoyed about it.
I hate pointing fingers because I understand the limits of current medical education and practice. But I truly feel like many of my best years were spent actively ignoring my own intuition because I was told, over and over, that I was “sick” and that I had to “listen” to professionals. I was pushed to override my higher self and inner guidance, which led to multiple emotional breakdowns and deep questions about my sanity.
I often wonder: Who would I have been if I hadn’t been scrutinized so intensely—while others with similar or worse struggles never faced the same hurdles under the name of healthcare?
What We’re Asking For:
▶Mandatory Black Box Warning discussions before psychiatric drugs are prescribed
▶Required informed consent documentation outlining common and rare side effects
▶Routine pharmacogenetic testing made accessible and insurance-covered
▶Psychiatric alternatives education: therapy, nutrition, lifestyle, mindfulness, and trauma healing
▶Oversight into APA and pharmaceutical lobbying practices that influence treatment standards
This Is Not Anti-Medication. It’s Pro-Choice, Pro-Informed Consent, and Pro-Safety.
▶No one should be prescribed life-altering medications without understanding the risks. No teenager should feel suicidal from a pill meant to help them. No family should suffer the consequences of chemical reactions ignored or denied.
▶Let’s build a future where psychiatric care is truly patient-centered, science-driven, and accountable.
▶If you’ve ever felt harmed, misled, or rushed into psychiatric medication without full information—please sign and sharethis petition.
▶Together, we can demand the safety, dignity, and truth that every patient deserves.
Seek and you shall find. When you walk into a psychiatrist’s office and share your struggles, their job—by design—is often to provide a diagnosis or a prescription. Similarly, therapists trained within certain clinical frameworks will typically offer a DSM-based diagnosis.
I’m not saying these approaches are incorrect or that the science behind them is invalid. But I do believe there’s more to mental health than what fits neatly into a diagnostic manual or a pill bottle. Anything too rigid or one-size-fits-all is a red flag to me.
Mental health care should honor the complexity of each individual’s experience, intuition, and healing journey—not just checkboxes and scripts.
The New Standard: We must move away from a blanket, one-size-fits-all approach that hands out potentially life-altering and personality-altering medications as a first step. Mental health treatment should be personalized, cautious, and centered on informed choice—actively avoiding unnecessary or premature medication whenever possible.
I often reference the Amen Clinics because I really appreciate their philosophy. Their approach focuses on helping patients understand their brain health and, when possible, reducing reliance on multiple psychiatric medications. In some of their books, they’ve shared stories of people who came to them as a last resort—often overwhelmed and barely functioning after being placed on 15 or more medications over time. Despite the cost, these individuals sought real answers and support, and the clinic’s goal was to offer a clearer path to healing.
See 🙏:
https://www.change.org/p/psychotropic-drugs-waiver-madi-s-law/u/33007758
"She was hospitalized two weeks before her death for adverse reaction to lexapro and lorazepam (the family Doctor gave her). These drugs caused suicidal ideation. Despite this there was no family meeting and the Doctors continued on with the drugs that led to her death by suicide."

210
The Issue
To: U.S. Congress, FDA, American Psychiatric Association, and Mental Health Providers Nationwide
We, the undersigned, call for an immediate reevaluation of psychiatric drug prescribing practices. This includes:
▶Transparent, mandatory disclosure of Black Box warnings
▶Routine offering of pharmacogenetic testing (e.g., GeneSight)
▶Informed consent policies that fully educate patients—especially youth—on potential risks
▶Greater emphasis on alternatives to medication-first approaches in mental health care
My Story: A Cautionary Tale of Blind Trust in the System
At just 16, I was forcibly placed on psychiatric medications including Lexapro, Wellbutrin, Adderall, and later Klonopin. I trusted the professionals who said it was the best path forward for my specific issues that only snowballed the more time I spent in their care. But instead of feeling better, I spiraled into unfamiliar emotional states, losing touch with my inner compass. It wasn’t until 2019, when I stopped taking them entirely and transitioned to PRNs and a different type of protocol only, that I truly started to recover. With some expected hiccups due to a recent head injury.
I’m not here to vilify doctors. They did what they believed was right with the education they had. But I believe there's a bigger truth being ignored: psychiatric medications are not for everyone, and in my case, they caused more harm than good. I later found out through a gene sight test that many of the drugs my therapist said "she would stop seeing me for if I didn't take" I was actually highly allergic to and was taking for years!!!
The sad truth? Sometimes you’re prescribed a drug for depression or lack of focus, only to become so wired that you then need medication for anxiety. Over time, you lose touch with your natural rhythms—feeling both wired and exhausted—and need an “off/on switch via a pill” just to function. When that switch stops working, doctors often add new layers of medication to “top you off” and treat the symptoms caused by previous drugs.
Mix that with occasional alcohol or cannabis use, and over time you’re creating a recipe for a potential psychotic breakdown. What late teen or young adult struggling with depression doesn’t sometimes use these substances—whether it’s “hanging out with friends” or trying to appear “normal,” even while knowing deep down that mixing recreational drugs with prescribed medications can lead to irreversible consequences? Some of these consequences are so serious they can even lead to arrest. Many people don’t realize why their personality or behavior has changed. It’s incredibly difficult to be fully self-aware of these shifts—especially if you’re isolated or simply living through the experience. Expecting someone who is unwell, injured and cycling in and out of episodes to step back and objectively observe themselves isn’t fair. Asking them to have insight into their condition while they are still in the midst of it—and then holding them accountable for that lack of insight—raises serious ethical concerns.
This is how severe the risks are. When these behavioral changes happen, people often blame it solely on the recreational substances—“It’s the pot,” they say—but rarely do they consider the role of the prescribed pills. The medication’s impact is too often overlooked. If you speak out about these issues, you’re often dismissed as a conspiracy theorist or accused of being anti-science...a bad influence. People who swear by their medications sometimes tell you to stay quiet because the drugs “saved their life.” And that’s great—if it worked for you, I’m truly glad. But it didn’t work for me, and my experience deserves to be heard—because there are others out there who feel too isolated or afraid to speak up against the mainstream expectations around medication and mental health. Too often, the moment someone “appears not to be doing well,” the first question asked is, “Are you taking your meds?” as if nothing else could possibly be causing their struggles.
For starters, let’s consider the economic fallout of long-term mental health challenges—and the soul-crushing weight of realizing that your life’s trajectory has shifted dramatically from what your younger self once expected. As a teen, everyone assumed you’d do well in life, but after years of taking psychiatric medications, your adult reality feels far from that hope. It’s like the classic chicken-or-egg question: did the reckless behavior come from taking drugs that caused excessive energy—like Adderall or Wellbutrin—or was it the weekend beers and cannabis? Why is it that you never craved cannabis or alcohol until you started those excitatory medications? And how did Lexapro dull your emotions so much that you felt you needed those substances just to have a conversation, instead of feeling like a blank mute?
One can’t help but wonder if many of the choices or life decisions made would have been more in alignment with who someone was before all of this mental health intervention and analysis, rather than after. The person I was before would have been far more careful, while the person I became afterward was much more reckless.
Not much thought is given—or at least not explained in layman’s terms—about the long-term impacts of starting these drugs early, just as the brain’s scaffolding and prefrontal cortex are still developing and strengthening. It makes sense, then, that questioning these treatments isn’t crazy or ludicrous. No one explains what happens if you stop taking a drug you’ve been primed to rely on—even after realizing it wasn’t good for you. Maybe it’s because they don’t have clear official guidance on how to manage that process yet.
Most therapists or experts will say, “These drugs are proven to HELP, and they can REVERSE the effects of depression, which we KNOW you have based on this 5-minute questionnaire.” That diagnosis can then define your whole identity for life and pressure you into believing how crucial the medication is—forever. But it’s also important to remember that this framing is part of their job.
Is it fair to blame all of this solely on the meds or the mental health system? Certainly not—it’s a complex, multifaceted issue. But it’s absolutely reasonable to recognize medication mismanagement and physiological incompatibility as a significant contributing factor in that difficult journey.
What’s a boon for someone else can be a bane for you.
The increase in prescribing antipsychotics over the past 7–10 years has led to a rise in side effects like tremors—symptoms that once were less common. Some treatment centers even resort to ECT (electroconvulsive therapy), despite repeated evidence of serious, long-lasting side effects.
What Are Black Box Warnings?
▶Black Box Warnings are the FDA’s most serious alert for prescription drugs, highlighting risks of serious, life-threatening adverse effects, such as:
▶Suicidal ideation (especially in teens and young adults)
▶Increased aggression
▶Severe withdrawal symptoms
▶Long-term neurological impacts
▶SSRIs (like Prozac), SNRIs, benzodiazepines, and antipsychotics often carry such warnings—but these are rarely explained properly to patients.
Emotional numbing and reduced empathy can be side effects associated with some psychotropic medications, including those with black box warnings. Here's how:
▶Emotional numbing (or emotional blunting) is commonly reported with many antidepressants, especially SSRIs like fluoxetine (Prozac), sertraline (Zoloft), and escitalopram (Lexapro).
▶Patients often describe feeling less able to experience a full range of emotions—both positive and negative—which can feel like a “flattening” or “numbing” effect.
▶Reduced empathy is less commonly discussed but has been reported anecdotally and in some studies. Some people on certain antidepressants or antipsychotics report feeling more detached from others emotionally, which can impact social relationships.
▶Antipsychotics may also contribute to emotional blunting or diminished affect as part of their sedative and dopamine-blocking effects.
▶These effects are not universal, but they are recognized enough to be concerns discussed in psychiatric and patient communities.
Sources in a numbered list for easy reference:
▶University of Cambridge study on emotional blunting caused by antidepressants
https://www.cam.ac.uk/research/news/scientists-explain-emotional-blunting-caused-by-common-antidepressants
▶Psychiatrist.com article on why antidepressants cause emotional blunting
https://www.psychiatrist.com/news/why-antidepressants-cause-emotional-blunting/
▶Study on antidepressants reducing pain empathy (Translational Psychiatry)
https://pubmed.ncbi.nlm.nih.gov/31175273/
▶Qualitative study on emotional blunting from long-term antipsychotic use
https://journals.kmanpub.com/index.php/prien/article/view/3341
▶British mental health charity Mind on antipsychotics and side effects
https://www.mind.org.uk/information-support/drugs-and-treatments/antipsychotics/side-effects/
Furthermore, many psychotropic medications—especially certain antipsychotics and some mood stabilizers—are linked to serious physical health risks such as metabolic syndrome, which includes weight gain, diabetes, high blood pressure, and increased risk of heart disease. These side effects can drastically affect overall health and quality of life, yet they are often downplayed or not fully explained to patients before starting treatment.
The most serious concern of all is the risk of suicidal ideation and aggressive behavior, particularly among adolescents and young adults. The FDA has issued black box warnings for certain antidepressants, indicating an increased risk of suicidal thoughts and behaviors in this age group.
While some studies have investigated potential links between psychiatric medications and violent incidents, such as school shootings, the findings are complex and not definitive. For instance, a study published in Behavioral Sciences & the Law found that most school shooters were not previously treated with psychotropic medications, and no direct or causal association was established.
However, individual cases have raised concerns. For example, Eric Harris, one of the perpetrators of the Columbine High School massacre, was prescribed fluvoxamine (Luvox), an SSRI antidepressant. Additionally, the shooter in the 2008 Northern Illinois University incident had been prescribed Prozac, Xanax, and Ambien, and reportedly stopped taking Prozac shortly before the event.
These instances underscore the importance of careful monitoring and informed decision-making when prescribing psychotropic medications, especially to young individuals. It's crucial to balance the benefits of treatment with the potential risks, ensuring that patients and their families are fully informed.
Starting or stopping psychiatric medications suddenly can cause serious, even dangerous, side effects. Here’s why, especially when it comes to things like aggression, violence, or even death:
1. Brain Chemistry Disruption
▶Psych meds (like antidepressants, antipsychotics, mood stabilizers, benzodiazepines, stimulants, etc.) work by altering neurotransmitters—like serotonin, dopamine, norepinephrine, and GABA. These chemicals regulate mood, impulse control, anxiety, and more.
▶When you stop suddenly, the brain is thrown into chemical chaos. It has adjusted to the medication and needs time to recalibrate. Without that transition, things can go very wrong—fast.
2. Withdrawal vs. Relapse vs. Rebound Effects
▶Withdrawal: Your brain struggles without the drug it's used to, sometimes mimicking or worsening the symptoms it was treating.
▶Relapse: The original condition may come back stronger.
▶Rebound: Some symptoms (like anxiety or insomnia) can come back even worse than before—often temporarily—but severely.
This can lead to:
▶Severe irritability or rage
▶Impulsivity or agitation
▶Paranoia or panic
▶Suicidal or homicidal thoughts in extreme cases
3. Benzodiazepines and Antidepressants Are Particularly Risky
▶Benzodiazepines (e.g., Xanax, Ativan): Stopping suddenly can cause seizures, psychosis, or extreme aggression.
▶SSRIs/SNRIs (e.g., Zoloft, Effexor): Can cause “SSRI discontinuation syndrome” — brain zaps, depersonalization, mood swings, etc.
▶Antipsychotics: Sudden withdrawal can cause rebound psychosis or mania.
4. Every Brain Is Different
Some people might feel just a little weird, others might feel like they’re losing control or becoming a different person. Underlying mental health conditions can be exacerbated, like a head injury/post concussive syndrome/TBI (Traumatic Brain Injury), and emotional regulation can become seriously impaired.
5. Why It Can Turn Violent
▶The frontal lobe (responsible for decision-making and impulse control) is often already compromised in psychiatric conditions.
▶Rapid withdrawal or incorrect dosing can impair it further.
▶That’s why stories of sudden violence (including self-harm or harm to others) are linked in rare—but real—cases of abrupt medication changes.
▶The frontal lobe—especially the prefrontal cortex—is deeply involved in many psychiatric conditions. It plays a key role in decision-making, emotional regulation, impulse control, motivation, and social behavior. When psychiatric conditions affect this region, it can lead to many of the symptoms we associate with mental illness.
Here’s a breakdown:
🧠 What Does the Frontal Lobe Do?
▶Executive function: planning, organizing, prioritizing
▶Impulse control: stopping inappropriate behaviors
▶Emotional regulation: managing mood and reacting appropriately
▶Social behavior: empathy, moral reasoning, understanding consequences
▶Attention and focus
▶Motivation and initiative
🔥 How It’s Affected in Psychiatric Conditions
1. Depression
Underactivity in the dorsolateral prefrontal cortex
This leads to:
▶Poor concentration and planning
▶Lack of motivation
▶Difficulty making decisions
▶Emotional flatness or excessive guilt
2. ADHD
Impaired function of the prefrontal cortex
Leads to:
▶Impulsivity
▶Poor attention
▶Difficulty with delayed gratification
3. Bipolar Disorder
During mania: frontal lobe activity decreases, leading to:
▶Poor judgment
▶Risk-taking behavior
▶Grandiosity
▶During depression: similar to MDD, with hypoactivity in frontal circuits
4. Schizophrenia
Hypofrontality—reduced blood flow and activity in the frontal lobe
Causes:
▶Disorganized thinking
▶Poor insight
▶Impaired executive function
▶Emotional blunting
5. PTSD
▶Disrupted communication between the prefrontal cortex and amygdala
▶The amygdala becomes hyperactive (fear), while the frontal lobe fails to properly inhibit it
Result: heightened emotional reactivity and poor regulation
6. Substance Use Disorders
Chronic use of drugs (especially stimulants, alcohol, or opioids) impairs frontal lobe function
Leads to:
▶Impaired judgment
▶Impulsivity
▶Craving cycles and relapse behavior
🧪 Brain Imaging Evidence
Technologies like fMRI and SPECT scans (which Amen Clinics uses) show that people with psychiatric disorders often have:
▶Decreased blood flow to frontal regions
▶Reduced gray matter volume
▶Disrupted connectivity between frontal areas and emotional centers like the limbic system
🔄 Why This Matters for Behavior
When the frontal lobe is compromised, a person may:
▶Struggle to regulate emotions (e.g., sudden outbursts)
▶Make poor or risky decisions
▶Act impulsively without considering consequences
▶Feel “flat” or overly reactive
▶This is one reason why med changes, trauma, or stress can push someone into a dangerous state—they're already operating with reduced “brakes,” and when emotional “gas pedals” like the amygdala kick in, it can overwhelm their ability to self-regulate.
What to Do:
▶Never stop psychiatric meds cold turkey without medical supervision.
▶Taper slowly under a doctor’s guidance.
▶Report any sudden mood changes immediately.
💥 Why Starting or Stopping Psych Meds Suddenly Can Lead to Violence, Rage, or Even Death
It sounds extreme, but sudden changes in psychiatric medication — especially stopping "cold turkey" — can absolutely lead to severe side effects like aggression, violence, psychosis, and in rare cases, suicide or death. One of the most alarming contributors to this is a condition called akathisia.
🧠 The Brain on Psych Meds
Psych medications affect neurotransmitters—chemicals that control mood, energy, anxiety, impulse control, sleep, and more. Over time, your brain adjusts to the presence of these drugs.
Suddenly removing or drastically altering them doesn’t give the brain time to adapt. The result? A chaotic chemical imbalance that can lead to:
▶Extreme agitation
▶Mood swings
▶Paranoia
▶Impulse control loss
▶Intense restlessness or anxiety
🚨 What Is Akathisia?
Akathisia is a movement and mental restlessness disorder often caused by starting, stopping, or changing the dose of antipsychotics, SSRIs, or other psych drugs.
Symptoms:
▶A feeling of being trapped inside your own skin
▶Compulsive pacing, rocking, or leg movement
▶Intense internal torment
▶Inability to sit still
▶Rage or suicidal thoughts driven by mental agony
▶People with akathisia often feel like they're going insane. They may appear agitated or hostile. Tragically, many cases of sudden suicide or violence following medication changes have been linked to undiagnosed akathisia.
📉 Withdrawal, Rebound, and Relapse
When people stop psych meds suddenly:
▶Withdrawal kicks in (shakes, insomnia, anxiety, confusion).
▶Rebound symptoms can be worse than the original condition (e.g., panic, depression, mania).
▶Relapse of the underlying illness can occur fast—and more severely.
▶Combined, this creates a perfect storm for dangerous behavior, especially if akathisia is part of the picture.
⚠️ Real-World Examples
▶SSRIs (like Paxil or Zoloft): Discontinuation can cause akathisia, panic attacks, electric shock sensations, and aggression.
▶Antipsychotics (like Abilify or Risperdal): Sudden withdrawal can lead to psychosis, akathisia, or even catatonia.
▶Benzodiazepines (like Xanax or Klonopin): Cold-turkey withdrawal can cause seizures, psychotic breaks, and violent outbursts.
✅ What to Do Instead
▶Always taper slowly under medical supervision—especially with meds like SSRIs, SNRIs, antipsychotics, and benzos.
▶Watch for signs of akathisia—especially after dose changes.
▶Be honest with your doctor about side effects—agitation is not just “anxiety.”
▶If you or someone else feels “not in control” after a med change, get help immediately. Time matters.
⚠️ Why Gabapentin and Stimulants (like Adderall) Can Be Dangerous
🔹 Gabapentin (Neurontin)
Originally approved for seizures, gabapentin is now commonly prescribed off-label for anxiety, insomnia, pain, and more. But it’s not without risk:
🚨 Dangers of Gabapentin:
▶Sedation + respiratory depression when combined with opioids, benzos, or alcohol (can be fatal)
▶Withdrawal effects: stopping suddenly can cause anxiety, agitation, insomnia, tremors—even seizures
▶Mood instability: some report increased suicidal thoughts, hostility, or mania (especially with bipolar)
▶Dependence: despite not being a controlled substance everywhere, it’s increasingly abused for its calming or euphoric effects
▶Cognitive dulling: can cause "brain fog," slowness, or affect memory
🧠 Frontal Lobe Impact:
▶Can dampen excitatory brain activity, leading to emotional flattening, impulsivity, or disinhibition in some
▶May interfere with mood regulation, especially if taken long-term or in high doses
🔹 Stimulants (e.g., Adderall, Ritalin, Vyvanse)
▶These are amphetamines or methylphenidate-based meds used for ADHD. When carefully prescribed, they can improve focus and impulse control. But they carry serious risks, especially when:
▶Overused
▶Mixed with other drugs
▶Taken without ADHD
▶Stopped abruptly
🚨 Dangers of Stimulants:
▶Increased heart rate and blood pressure — raises risk for stroke, arrhythmias, even sudden death in vulnerable individuals
▶Anxiety, panic, or paranoia (especially at high doses or when sleep-deprived)
▶Mania or psychosis in people with bipolar or schizophrenia
▶Aggression and impulsivity — overstimulation of the brain’s “go” systems can override normal self-control
▶Crash and rebound depression when the drug wears off or is suddenly stopped
▶Addiction risk: Adderall is a Schedule II controlled substance for a reason — tolerance builds, and misuse can spiral quickly.
🧠 Frontal Lobe Impact:
Stimulants intensify dopamine and norepinephrine in the prefrontal cortex — which improves focus short-term but can:
▶Overload emotional regulation
▶Trigger rage, obsessive behavior, or paranoia
▶Impair long-term balance in brain reward circuits
❗When Combined (or Used Without a Clear Diagnosis)
Using gabapentin + stimulants, or either one in someone with undiagnosed bipolar, trauma, or psychotic risk, can be a recipe for disaster:
▶May cause emotional instability, outbursts, panic, or aggression
▶Masks symptoms instead of addressing the root cause
▶May be seen as “safe” — leading to under-monitoring and dangerous self-medication or withdrawal
🔄 Key Rule: Start low, go slow, taper gently, and monitor carefully.
Just because a drug is common doesn't mean it's harmless. Your brain is a finely tuned system — even small shifts in neurotransmitters can dramatically change behavior, perception, and mood.
Varenicline (Chantix) and bupropion (Wellbutrin, also called Budeprion) are essentially the same chemical compound. There is a significant difference between Wellbutrin XL (extended-release) and Wellbutrin SR (short-release). About seven years ago, there was a recall involving this medication. Both starting and abruptly stopping Wellbutrin can increase the risk of seizures.
What’s interesting is that this is a clear example of rebranding and off-label use—where the same substance is packaged and promoted for entirely different purposes. For example, bupropion was originally developed as an antidepressant (Wellbutrin), but later rebranded for smoking cessation (Chantix). Similarly, Vyvanse, a stimulant approved for ADHD, was also marketed for binge eating disorder—despite the fact that it can be particularly risky or easily abused by individuals with a history of eating disorders.
- Fluoxetine (Prozac) and Workplace Violence
In 1989, Joseph T. Wesbecker killed eight people and injured twelve before committing suicide. He had begun taking fluoxetine (Prozac) 11 days prior. His relatives and victims attributed his actions to the medication, leading to a lawsuit against the manufacturer, Eli Lilly, which settled for $50 million across 300 claims. Internal documents revealed that fluoxetine had been linked to suicide attempts during clinical trials, raising concerns about its safety.
2. Maharishi University of Management Stabbing
In 2004, a student at Maharishi University of Management in Iowa fatally stabbed a fellow student. The perpetrator, diagnosed with schizophrenia, had been off his medication for months at the time of the incident. He was later found not guilty by reason of insanity, highlighting the potential risks of discontinuing psychiatric medication.
3. Antidepressant-Induced Violence
Studies have shown that certain antidepressants, such as venlafaxine (Effexor) and fluvoxamine (Luvox), are more likely to be associated with violent behavior compared to other drugs. For instance, venlafaxine is 8.3 times more likely to be linked with violence than other medications .
4. Benzodiazepine Abuse and Aggression
Flunitrazepam, a benzodiazepine, has been implicated in cases of extreme aggression and violence. Forensic psychiatric patients who abused flunitrazepam exhibited violent behavior, lack of empathy, and impaired judgment, often in combination with alcohol or other drugs .
5. 25I-NBOMe and Hallucinogenic-Induced Violence
25I-NBOMe, a synthetic hallucinogen, has been linked to several violent incidents. In 2015, a 20-year-old student in California died after consuming 25I-NBOMe and engaging in a violent episode. In the UK, a teenager fatally stabbed his friend during a psychotic episode induced by the drug .
(I’ve gone back to my old pharmacy and obtained all records from when I first started taking medications—going back as far as possible—and I’ve been prescribed nearly all of these drugs except five and two. That tells me a lot, including how early and easily doctors, who clearly just saw me as someone to get in and out of their office, were willing to prescribe serious medications without knowing anything meaningful about who I was or the impact of these drugs on my life)
Here's a list of common psychiatric and mental health medications that carry FDA Black Box Warnings—the strongest warning the FDA issues. These warnings highlight serious or life-threatening risks such as suicidal ideation, addiction, withdrawal, respiratory depression, or irreversible side effects.
⚠️ BLACK BOX WARNED PSYCHIATRIC DRUGS:
🧠 Antidepressants (SSRIs, SNRIs, TCAs, MAOIs)
All antidepressants approved for depression carry a Black Box Warning for:
▶Increased risk of suicidal thinking and behavior in children, adolescents, and young adults (up to age 24).
Examples:
▶Fluoxetine (Prozac)
▶Sertraline (Zoloft)
▶Citalopram (Celexa)
▶Escitalopram (Lexapro)
▶Paroxetine (Paxil)
▶Venlafaxine (Effexor)
▶Duloxetine (Cymbalta)
▶Desvenlafaxine (Pristiq)
▶Amitriptyline (Elavil)
▶Nortriptyline (Pamelor)
▶Bupropion (Wellbutrin) – Also carries seizure risk warning.
💊 Benzodiazepines (Anti-anxiety, Sedative)
In 2020, the FDA added a Black Box Warning to all benzodiazepines:
Serious risks of abuse, misuse, addiction, physical dependence, and withdrawal reactions—even when used as prescribed.
Examples:
▶Alprazolam (Xanax)
▶Clonazepam (Klonopin)
▶Lorazepam (Ativan)
▶Diazepam (Valium)
▶Temazepam (Restoril)
⚡ Stimulants (ADHD medications)
Many stimulants used to treat ADHD carry Black Box Warnings for:
▶High potential for abuse and dependence; sudden cardiac death or serious cardiovascular events; psychiatric adverse events (mania, aggression, psychosis).
Examples:
▶Adderall (amphetamine/dextroamphetamine)
▶Ritalin (methylphenidate)
▶Concerta (methylphenidate ER)
▶Vyvanse (lisdexamfetamine)
▶Dexedrine (dextroamphetamine)
🧩 Antipsychotics (Typical & Atypical)
Most antipsychotics carry Black Box Warnings for:
▶Increased mortality in elderly patients with dementia-related psychosis.
▶Some also warn of metabolic side effects, movement disorders (e.g., tardive dyskinesia), and neuroleptic malignant syndrome.
Examples:
▶Risperidone (Risperdal)
▶Olanzapine (Zyprexa)
▶Quetiapine (Seroquel)
▶Aripiprazole (Abilify)
▶Ziprasidone (Geodon)
▶Haloperidol (Haldol)
▶Lurasidone (Latuda)
▶Clozapine (Clozaril) – Also has a unique black box warning for agranulocytosis (fatal blood disorder), seizures, and myocarditis.
🧬 Mood Stabilizers & Anticonvulsants (often used for Bipolar Disorder)
Some mood stabilizers and anticonvulsants have Black Box Warnings for:
Suicidal behavior and ideation and life-threatening skin reactions (like Stevens-Johnson syndrome).
Examples:
▶Lamotrigine (Lamictal)
▶Valproic acid / Divalproex (Depakote) – also has warning for hepatotoxicity, teratogenicity, pancreatitis
▶Carbamazepine (Tegretol)
▶Oxcarbazepine (Trileptal) – similar risks
When the System Fails the Vulnerable
There are haunting real-world consequences when risks are ignored. One such case is that of a woman in Virginia who, just days after being prescribed Prozac, took her own life and the lives of her children. These tragic outcomes are too often brushed under the rug by pharmaceutical companies and professional boards like the APA.
Documentaries like “Psychiatry: An Industry of Death” highlight the historical and ongoing collusion between pharma and psychiatry, raising red flags about overdiagnosis, overmedication, and profit-driven treatment models. This documentary is highly controversial and has faced significant public backlash—first, due to its association with Scientology propaganda, and second, because many believe it promotes harmful views that undermine modern, evidence-based mental health care. However, having watched it twice, I found that it presents an alternative perspective on mental health—one that, while unsettling, offers insight into its historical roots and raises important questions that are often overlooked.
Source: https://www.cchr.org/quick-facts/introduction.html
Why Aren’t We Using Tools Like GeneSight?
Pharmacogenetic testing has been available since 2011. These tests analyze how your unique DNA may influence your response to medications—helping avoid dangerous side effects. Yet, most mental health providers never mention it, especially in insurance-based clinics.
Wouldn’t you want to know which drugs your body is genetically incompatible with before putting them in your system?
The Bigger Picture: A Chemical Trap
Mental health is not one-size-fits-all. Yet the industry often treats psych drugs as the only viable solution. Antipsychotics, for instance, are increasingly prescribed—even off-label—despite severe risks like metabolic syndrome, tardive dyskinesia, and lifelong dependency. Patients are rarely warned about these outcomes.
Many are discouraged from questioning their prescriptions. I remember being told things when I was in my early twenties like, “Oh stop, you’re too pretty to be sad just smile!,” or “You just need a chemical fix.” But my struggles weren’t superficial—they were deeply personal and increasingly chemical, because of the drugs themselves.
Oftentimes, patients are told that the risk of serious side effects is clinically marginal—that statistically, it "would never be you." Well, guess what? It was me. And honestly, I’m still kind of annoyed about it.
I hate pointing fingers because I understand the limits of current medical education and practice. But I truly feel like many of my best years were spent actively ignoring my own intuition because I was told, over and over, that I was “sick” and that I had to “listen” to professionals. I was pushed to override my higher self and inner guidance, which led to multiple emotional breakdowns and deep questions about my sanity.
I often wonder: Who would I have been if I hadn’t been scrutinized so intensely—while others with similar or worse struggles never faced the same hurdles under the name of healthcare?
What We’re Asking For:
▶Mandatory Black Box Warning discussions before psychiatric drugs are prescribed
▶Required informed consent documentation outlining common and rare side effects
▶Routine pharmacogenetic testing made accessible and insurance-covered
▶Psychiatric alternatives education: therapy, nutrition, lifestyle, mindfulness, and trauma healing
▶Oversight into APA and pharmaceutical lobbying practices that influence treatment standards
This Is Not Anti-Medication. It’s Pro-Choice, Pro-Informed Consent, and Pro-Safety.
▶No one should be prescribed life-altering medications without understanding the risks. No teenager should feel suicidal from a pill meant to help them. No family should suffer the consequences of chemical reactions ignored or denied.
▶Let’s build a future where psychiatric care is truly patient-centered, science-driven, and accountable.
▶If you’ve ever felt harmed, misled, or rushed into psychiatric medication without full information—please sign and sharethis petition.
▶Together, we can demand the safety, dignity, and truth that every patient deserves.
Seek and you shall find. When you walk into a psychiatrist’s office and share your struggles, their job—by design—is often to provide a diagnosis or a prescription. Similarly, therapists trained within certain clinical frameworks will typically offer a DSM-based diagnosis.
I’m not saying these approaches are incorrect or that the science behind them is invalid. But I do believe there’s more to mental health than what fits neatly into a diagnostic manual or a pill bottle. Anything too rigid or one-size-fits-all is a red flag to me.
Mental health care should honor the complexity of each individual’s experience, intuition, and healing journey—not just checkboxes and scripts.
The New Standard: We must move away from a blanket, one-size-fits-all approach that hands out potentially life-altering and personality-altering medications as a first step. Mental health treatment should be personalized, cautious, and centered on informed choice—actively avoiding unnecessary or premature medication whenever possible.
I often reference the Amen Clinics because I really appreciate their philosophy. Their approach focuses on helping patients understand their brain health and, when possible, reducing reliance on multiple psychiatric medications. In some of their books, they’ve shared stories of people who came to them as a last resort—often overwhelmed and barely functioning after being placed on 15 or more medications over time. Despite the cost, these individuals sought real answers and support, and the clinic’s goal was to offer a clearer path to healing.
See 🙏:
https://www.change.org/p/psychotropic-drugs-waiver-madi-s-law/u/33007758
"She was hospitalized two weeks before her death for adverse reaction to lexapro and lorazepam (the family Doctor gave her). These drugs caused suicidal ideation. Despite this there was no family meeting and the Doctors continued on with the drugs that led to her death by suicide."
210

Supporter Voices
Petition Updates
Share this petition
Petition created on September 16, 2023