Include Complex PTSD (CPTSD) in the Next Edition of the DSM!

Include Complex PTSD (CPTSD) in the Next Edition of the DSM!
The Issue
What is the DSM?
The Diagnostic and Statistical Manual (DSM) is a guide to psychiatric diagnosis, designed by and for mental health professionals. Following the publication of the first version of the DSM in 1952, there have been multiple iterations of the DSM, the most recent being the DSM-V-TR, which came out in 2022. The DSM is organized into categories of disorders; these categories each contain a number of specific diagnoses; and specific symptoms/criteria for making each diagnosis are listed within each specific diagnosis. (Each diagnosis also has a lettered and numbered “code,” in addition to a name.) Mental health practitioners use DSM criteria to diagnose their clients. When mental health practitioners take insurance, services such as therapy typically can only be covered by insurance if the patient has a DSM diagnosis (or a diagnosis recognized by another diagnostic guide, called the International Classification of Diseases, or ICD).
In other words, for mental health care to be covered by insurance, the patient’s “need for these services and pharmaceuticals must be deemed medically necessary, which requires a diagnosis,” as an article in Forbes puts it (Martin & Masterson, 2024).
What is Complex PTSD (C-PTSD), and how is it different from ‘traditional’ PTSD?
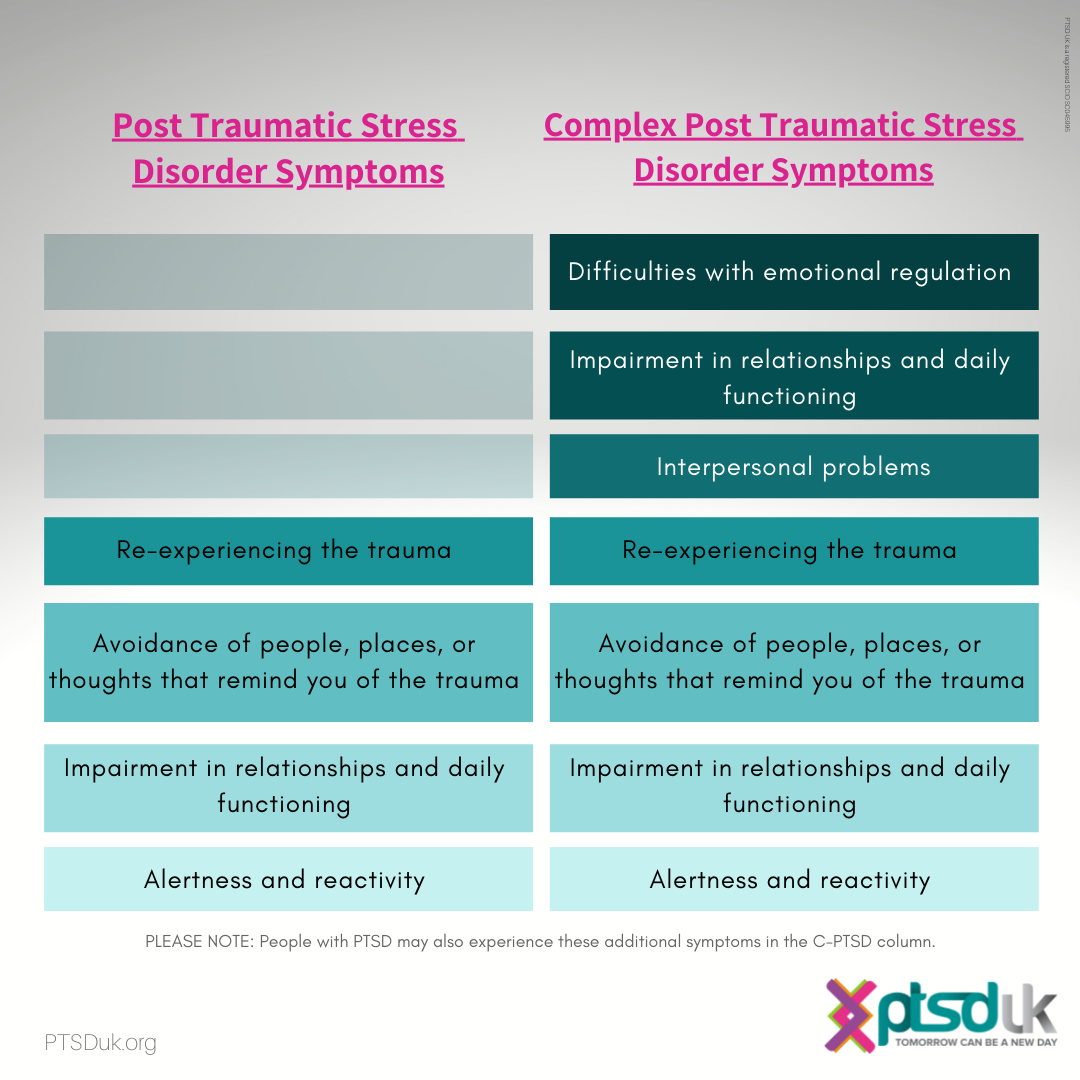
First proposed by Harvard psychiatrist Judith Herman, C-PTSD is intended to capture the specific experiences of people who have experienced chronic trauma, often in childhood, involving interpersonal relationships. Herman noticed that her patients who had such experiences (including, for instance, survivors of childhood physical and sexual abuse) showed some symptoms of PTSD, but also other symptoms that were not included in that diagnosis.
According to the CPTSD Foundation, CPTSD “describes the results of ongoing, inescapable, relational trauma.” Moreover, whereas the existing PTSD is often associated with a single, distinct, traumatic event that triggers lasting symptoms, CPTSD describes symptoms that arise from a chain of traumatic events over an extended period of time (CPTSD Foundation).
Some of the hallmark differences between diagnoses include CPTSD’s impact on emotional regulation and interpersonal relationships. Individuals with CPTSD struggle with regulating mood and emotion, often feel intense guilt and shame, and have difficulty maintaining personal relationships as a result of their sustained interpersonal trauma.
Why add CPTSD to the DSM?
Crucially, therapeutic services can often be covered by insurance when an individual has a recognized DSM diagnosis. Insurance coverage can of course make mental healthcare vastly more accessible and affordable to patients. Additionally, diagnoses can at times be highly validating and affirming – giving individuals language to describe what they are experiencing, reminding them that they are not alone in their symptoms, and helping make clear that symptoms are not somehow personal to an individual or the “fault” of an individual. In the mental health context specifically, diagnoses can also serve as a reminder that mental health issues are just as real as physical health issues. Furthermore, recognizing CPTSD in the DSM might pave the way for individuals diagnosed with the condition to connect with one another (e.g., through support groups, etc.) and find community and common ground.
In the absence of a specific CPTSD diagnosis in the DSM, patients who would meet the criteria for CPTSD may instead be diagnosed with other conditions (such as the existing PTSD diagnosis, etc.) that do not reflect their symptoms as accurately. The diagnosis might in turn shape the course of treatment for these patients, and if the diagnosis is inaccurate, the treatment might be less effective. The recognition of C-PTSD might also spur more research regarding the symptoms of CPTSD and effective treatments, which could potentially benefit patients greatly over the longer term.
The other major, accepted diagnostic guide, the ICD, already recognizes CPTSD.
Why might some stakeholders disagree?
“Critics of the distinction of cPTSD have stated that it is unprecedented to grant a distinct diagnosis to a condition that is essentially a more severe form of a previously established diagnosis” (Cutlip et al., 2023). Complex PTSD “was not added as a separate diagnosis to the DSM-IV because results from the DSM-IV Field Trials indicated that 92% of individuals with complex PTSD… also met diagnostic criteria for PTSD” (U.S. Department of Veterans Affairs). While we recognize that there may be symptom overlap with PTSD - and with other diagnoses - it is important to note that overlap does not invalidate the existence of a separate condition. In fact, many conditions within the DSM hold similarities to one another, such as the irritability and impulsiveness seen in both BPD and Bipolar disorder. In the case of cPTSD, we have seen that the criteria describe unique facets around emotion regulation and interpersonal functioning. Because of this, we are comfortable with our assertion that cPTSD is still deserving of its own distinct diagnosis.
Additionally, some stakeholders may take issue with our push toward appealing to the DSM as an organization. Although the American Psychiatric Association describes the DSM as the “authoritative guide to the diagnosis of mental disorders,” not all mental health practitioners favor the usage of the DSM. Although the American Psychiatric Association describes the DSM as the “authoritative guide to the diagnosis of mental disorders,” not all mental health practitioners favor the usage of the DSM or specific updates that have been made to the DSM previously. Furthermore, historically, “formal” mental health diagnoses have often been used to stigmatize and strip power from some individuals experiencing a mental health concern. There is a rich history of black and brown individuals being diagnosed with psychotic disorders during protests that occurred around the civil rights movement, for example. While we recognize that the DSM is a flawed document - and that our petition may seem to “legitimize” the expert power of those who create it, we nevertheless believe this is a necessary step toward expanding treatment access for those who need it. It is an admirable goal to move away from the stigma and financial headaches embedded in the current diagnosis-required-for-treatment model, but that is not the reality of where our profession is at this current moment. As social workers, we believe we are obligated to not only work for future changes we would like to see happen in our world, but to work for our clients in the here-and-now. For this reason, we are taking this initial step to add cPTSD to the next iteration of the DSM.
References:
American Psychiatric Association (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). https://doi.org/10.1176/appi.books.9780890425787
American Psychiatric Association, (2024). “Frequently Asked Questions,” https://www.psychiatry.org/psychiatrists/practice/dsm/frequently-asked-questions
American Psychiatric Association, “Insurance Implications of DSM-5,” https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM_Insurance-Implications-of-DSM-5.pdf
Cloitre, M. (2020). ICD-11 complex post-traumatic stress disorder: simplifying diagnosis in trauma populations. The British Journal of Psychiatry, 216(3), 129–131. doi:10.1192/bjp.2020.43
Cutlip, H. A., Ang-Rabanes, M., & Mogallapu, R. (2023). Unknown, Underserved, Underreported: A Case for Differentiation in Trauma Disorder Classification and Diagnosis. Cureus, 15(5), e39157. https://doi.org/10.7759/cureus.39157
CPTSD Foundation, “What is Complex Post-Traumatic Stress Disorder? An information page on CPTSD (C-PTSD),” https://cptsdfoundation.org/what-is-complex-post-traumatic-stress-disorder-cptsd/
Frances, A. J., (2011, November 18). “Counselors Turn Against DSM 5,” Psychology Today. https://www.psychologytoday.com/us/blog/dsm5-in-distress/201111/counselors-turn-against-dsm-5
Martin, E., & Masterson, L., (2024, February 15). “Does insurance cover therapy?” Forbes. https://www.forbes.com/advisor/health-insurance/does-insurance-cover-therapy/
Metzl, J. (2011). The Protest Psychosis: How Schizophrenia Became a Black Disease. Beacon Press. https://www.amazon.com/Protest-Psychosis-Schizophrenia-Became-Disease/dp/0807001279
U.S. Department of Veteran Affairs . (2007, January 1). PTSD: National Center for PTSD. Complex PTSD. https://www.ptsd.va.gov/professional/treat/essentials/complex_ptsd.asp#:~:text=Although%20its%20inclusion%20was%20reconsidered,this%20was%20a%20separate%20diagnosis
See also:
1
The Issue
What is the DSM?
The Diagnostic and Statistical Manual (DSM) is a guide to psychiatric diagnosis, designed by and for mental health professionals. Following the publication of the first version of the DSM in 1952, there have been multiple iterations of the DSM, the most recent being the DSM-V-TR, which came out in 2022. The DSM is organized into categories of disorders; these categories each contain a number of specific diagnoses; and specific symptoms/criteria for making each diagnosis are listed within each specific diagnosis. (Each diagnosis also has a lettered and numbered “code,” in addition to a name.) Mental health practitioners use DSM criteria to diagnose their clients. When mental health practitioners take insurance, services such as therapy typically can only be covered by insurance if the patient has a DSM diagnosis (or a diagnosis recognized by another diagnostic guide, called the International Classification of Diseases, or ICD).
In other words, for mental health care to be covered by insurance, the patient’s “need for these services and pharmaceuticals must be deemed medically necessary, which requires a diagnosis,” as an article in Forbes puts it (Martin & Masterson, 2024).
What is Complex PTSD (C-PTSD), and how is it different from ‘traditional’ PTSD?
First proposed by Harvard psychiatrist Judith Herman, C-PTSD is intended to capture the specific experiences of people who have experienced chronic trauma, often in childhood, involving interpersonal relationships. Herman noticed that her patients who had such experiences (including, for instance, survivors of childhood physical and sexual abuse) showed some symptoms of PTSD, but also other symptoms that were not included in that diagnosis.
According to the CPTSD Foundation, CPTSD “describes the results of ongoing, inescapable, relational trauma.” Moreover, whereas the existing PTSD is often associated with a single, distinct, traumatic event that triggers lasting symptoms, CPTSD describes symptoms that arise from a chain of traumatic events over an extended period of time (CPTSD Foundation).
Some of the hallmark differences between diagnoses include CPTSD’s impact on emotional regulation and interpersonal relationships. Individuals with CPTSD struggle with regulating mood and emotion, often feel intense guilt and shame, and have difficulty maintaining personal relationships as a result of their sustained interpersonal trauma.
Why add CPTSD to the DSM?
Crucially, therapeutic services can often be covered by insurance when an individual has a recognized DSM diagnosis. Insurance coverage can of course make mental healthcare vastly more accessible and affordable to patients. Additionally, diagnoses can at times be highly validating and affirming – giving individuals language to describe what they are experiencing, reminding them that they are not alone in their symptoms, and helping make clear that symptoms are not somehow personal to an individual or the “fault” of an individual. In the mental health context specifically, diagnoses can also serve as a reminder that mental health issues are just as real as physical health issues. Furthermore, recognizing CPTSD in the DSM might pave the way for individuals diagnosed with the condition to connect with one another (e.g., through support groups, etc.) and find community and common ground.
In the absence of a specific CPTSD diagnosis in the DSM, patients who would meet the criteria for CPTSD may instead be diagnosed with other conditions (such as the existing PTSD diagnosis, etc.) that do not reflect their symptoms as accurately. The diagnosis might in turn shape the course of treatment for these patients, and if the diagnosis is inaccurate, the treatment might be less effective. The recognition of C-PTSD might also spur more research regarding the symptoms of CPTSD and effective treatments, which could potentially benefit patients greatly over the longer term.
The other major, accepted diagnostic guide, the ICD, already recognizes CPTSD.
Why might some stakeholders disagree?
“Critics of the distinction of cPTSD have stated that it is unprecedented to grant a distinct diagnosis to a condition that is essentially a more severe form of a previously established diagnosis” (Cutlip et al., 2023). Complex PTSD “was not added as a separate diagnosis to the DSM-IV because results from the DSM-IV Field Trials indicated that 92% of individuals with complex PTSD… also met diagnostic criteria for PTSD” (U.S. Department of Veterans Affairs). While we recognize that there may be symptom overlap with PTSD - and with other diagnoses - it is important to note that overlap does not invalidate the existence of a separate condition. In fact, many conditions within the DSM hold similarities to one another, such as the irritability and impulsiveness seen in both BPD and Bipolar disorder. In the case of cPTSD, we have seen that the criteria describe unique facets around emotion regulation and interpersonal functioning. Because of this, we are comfortable with our assertion that cPTSD is still deserving of its own distinct diagnosis.
Additionally, some stakeholders may take issue with our push toward appealing to the DSM as an organization. Although the American Psychiatric Association describes the DSM as the “authoritative guide to the diagnosis of mental disorders,” not all mental health practitioners favor the usage of the DSM. Although the American Psychiatric Association describes the DSM as the “authoritative guide to the diagnosis of mental disorders,” not all mental health practitioners favor the usage of the DSM or specific updates that have been made to the DSM previously. Furthermore, historically, “formal” mental health diagnoses have often been used to stigmatize and strip power from some individuals experiencing a mental health concern. There is a rich history of black and brown individuals being diagnosed with psychotic disorders during protests that occurred around the civil rights movement, for example. While we recognize that the DSM is a flawed document - and that our petition may seem to “legitimize” the expert power of those who create it, we nevertheless believe this is a necessary step toward expanding treatment access for those who need it. It is an admirable goal to move away from the stigma and financial headaches embedded in the current diagnosis-required-for-treatment model, but that is not the reality of where our profession is at this current moment. As social workers, we believe we are obligated to not only work for future changes we would like to see happen in our world, but to work for our clients in the here-and-now. For this reason, we are taking this initial step to add cPTSD to the next iteration of the DSM.
References:
American Psychiatric Association (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). https://doi.org/10.1176/appi.books.9780890425787
American Psychiatric Association, (2024). “Frequently Asked Questions,” https://www.psychiatry.org/psychiatrists/practice/dsm/frequently-asked-questions
American Psychiatric Association, “Insurance Implications of DSM-5,” https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM_Insurance-Implications-of-DSM-5.pdf
Cloitre, M. (2020). ICD-11 complex post-traumatic stress disorder: simplifying diagnosis in trauma populations. The British Journal of Psychiatry, 216(3), 129–131. doi:10.1192/bjp.2020.43
Cutlip, H. A., Ang-Rabanes, M., & Mogallapu, R. (2023). Unknown, Underserved, Underreported: A Case for Differentiation in Trauma Disorder Classification and Diagnosis. Cureus, 15(5), e39157. https://doi.org/10.7759/cureus.39157
CPTSD Foundation, “What is Complex Post-Traumatic Stress Disorder? An information page on CPTSD (C-PTSD),” https://cptsdfoundation.org/what-is-complex-post-traumatic-stress-disorder-cptsd/
Frances, A. J., (2011, November 18). “Counselors Turn Against DSM 5,” Psychology Today. https://www.psychologytoday.com/us/blog/dsm5-in-distress/201111/counselors-turn-against-dsm-5
Martin, E., & Masterson, L., (2024, February 15). “Does insurance cover therapy?” Forbes. https://www.forbes.com/advisor/health-insurance/does-insurance-cover-therapy/
Metzl, J. (2011). The Protest Psychosis: How Schizophrenia Became a Black Disease. Beacon Press. https://www.amazon.com/Protest-Psychosis-Schizophrenia-Became-Disease/dp/0807001279
U.S. Department of Veteran Affairs . (2007, January 1). PTSD: National Center for PTSD. Complex PTSD. https://www.ptsd.va.gov/professional/treat/essentials/complex_ptsd.asp#:~:text=Although%20its%20inclusion%20was%20reconsidered,this%20was%20a%20separate%20diagnosis
See also:
1
The Decision Makers
Petition Updates
Share this petition
Petition created on April 30, 2024