
Medical Software Glitch Masks Severe Lung Failure: Loophole Exposed
The issue
This petition is about an invisible hospital software flaw that is draining our healthcare budgets, leaving patients to silently suffocate, and trapping well-meaning doctors in catastrophic legal liabilities.
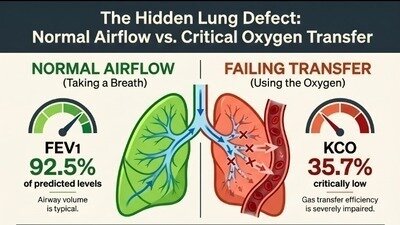
Right now, standard medical reporting systems favor a single metric: mechanical airflow volume (FEV1). If you are not constantly congested and can physically push air out of your lungs normally, a computer template automatically looks at that one number and stamps the entire report as "MILD" in bold letters right at the very top of the page.
But this is a life-threatening system error that hides severe organ failure.
Breathing isn't just about moving air in and out (airflow mechanics); it is about getting oxygen into your bloodstream (gas exchange). Because the software values exhalation over oxygen absorption, it completely ignores severe defects in deep lung tissues. In my case, while my exhalation was labeled "mild," my actual oxygen transfer coefficient (KCO) collapsed to extreme statistical limits, reaching a catastrophic Z-score of -5.79. during testing I gave it my all and it wasn't a machine error. The test was repeated several times to ensure complete accuracy, the equipment was fully calibrated, and the file was issued a flawless "Grade A" quality rating. The data is an undeniable physical fact.
Yet, here is the precise programming flaw that breaks the safety net: standard hospital software charts are only built to measure down to -5.6 on their visual graphs. Because my tissue failure was so extreme, my data point fell completely off the programmer's pre-set scale. Instead of triggering a massive, red-flag alert, the computer template stayed completely silent and buried the life-threatening defect, unmarked, at the very bottom of the page.
Modern doctors are under immense pressure, frequently managing complex cases in rapid 15-minute consultations. When a rushed clinician scans a report and sees a bold "Mild" stamp at the top, it creates an unintended cognitive trap. They trust the technology, close the file, and send the patient home. This means patients are left completely without vital oxygen treatments or medication for months on end sometimes receiving no medical help at all, while their organs deteriorate.
This glitch doesn't just destroy patient health—it breaks the clinical safety net.
Under national medical guidelines administered by AHPRA, a physician cannot pass legal liability over to a tech company when software templates get it wrong. Whether a patient files a formal negligence lawsuit, or an internal hospital clinical quality audit flags the error later during routine chart reviews, the individual treating doctor carries 100% of the blame for a system-generated blind spot. Relying blindly on an automated "Mild" summary does not shield a doctor from catastrophic career, regulatory, or legal crises. This software flaw actively sets dedicated practitioners up to fail.
Fixing this nightmare does not require millions of dollars, heavy equipment, or a healthcare overhaul. It takes a programmer less than a day and requires a simple, inexpensive conditional update to a few lines of computer programming code.
Our Unified Demand: Universal Top-Line Flagging.
We are calling on medical technology companies, hospital networks, and clinical safety boards to mandate a universal software rule: If any individual component of a respiratory report—whether it is airflow mechanics (FEV1), lung volumes (VA), or gas exchange (DLCO/KCO)—drops into a danger zone, the software must prominently flag it at the very top of the page. No computer system should ever be allowed to use a "mild" headline to mask an extreme, off-the-charts organ defect.
For Families: Sign this to ensure your mother, child, or partner is never turned away from life-saving treatment because a computer algorithm lied about their health.
For Doctors: Sign this to demand the accurate, high-visibility tools you need to protect your patients and shield your clinical practice from preventable legal crises.
Please sign and share this petition to close this invisible loophole once and for all. Your signature will force a tiny tech fix that will save thousands of lives and defend the healthcare workers who treat us.
👉 Click "Sign" now to fix the software flaw and protect patient safety 🫁

83
The issue
This petition is about an invisible hospital software flaw that is draining our healthcare budgets, leaving patients to silently suffocate, and trapping well-meaning doctors in catastrophic legal liabilities.
Right now, standard medical reporting systems favor a single metric: mechanical airflow volume (FEV1). If you are not constantly congested and can physically push air out of your lungs normally, a computer template automatically looks at that one number and stamps the entire report as "MILD" in bold letters right at the very top of the page.
But this is a life-threatening system error that hides severe organ failure.
Breathing isn't just about moving air in and out (airflow mechanics); it is about getting oxygen into your bloodstream (gas exchange). Because the software values exhalation over oxygen absorption, it completely ignores severe defects in deep lung tissues. In my case, while my exhalation was labeled "mild," my actual oxygen transfer coefficient (KCO) collapsed to extreme statistical limits, reaching a catastrophic Z-score of -5.79. during testing I gave it my all and it wasn't a machine error. The test was repeated several times to ensure complete accuracy, the equipment was fully calibrated, and the file was issued a flawless "Grade A" quality rating. The data is an undeniable physical fact.
Yet, here is the precise programming flaw that breaks the safety net: standard hospital software charts are only built to measure down to -5.6 on their visual graphs. Because my tissue failure was so extreme, my data point fell completely off the programmer's pre-set scale. Instead of triggering a massive, red-flag alert, the computer template stayed completely silent and buried the life-threatening defect, unmarked, at the very bottom of the page.
Modern doctors are under immense pressure, frequently managing complex cases in rapid 15-minute consultations. When a rushed clinician scans a report and sees a bold "Mild" stamp at the top, it creates an unintended cognitive trap. They trust the technology, close the file, and send the patient home. This means patients are left completely without vital oxygen treatments or medication for months on end sometimes receiving no medical help at all, while their organs deteriorate.
This glitch doesn't just destroy patient health—it breaks the clinical safety net.
Under national medical guidelines administered by AHPRA, a physician cannot pass legal liability over to a tech company when software templates get it wrong. Whether a patient files a formal negligence lawsuit, or an internal hospital clinical quality audit flags the error later during routine chart reviews, the individual treating doctor carries 100% of the blame for a system-generated blind spot. Relying blindly on an automated "Mild" summary does not shield a doctor from catastrophic career, regulatory, or legal crises. This software flaw actively sets dedicated practitioners up to fail.
Fixing this nightmare does not require millions of dollars, heavy equipment, or a healthcare overhaul. It takes a programmer less than a day and requires a simple, inexpensive conditional update to a few lines of computer programming code.
Our Unified Demand: Universal Top-Line Flagging.
We are calling on medical technology companies, hospital networks, and clinical safety boards to mandate a universal software rule: If any individual component of a respiratory report—whether it is airflow mechanics (FEV1), lung volumes (VA), or gas exchange (DLCO/KCO)—drops into a danger zone, the software must prominently flag it at the very top of the page. No computer system should ever be allowed to use a "mild" headline to mask an extreme, off-the-charts organ defect.
For Families: Sign this to ensure your mother, child, or partner is never turned away from life-saving treatment because a computer algorithm lied about their health.
For Doctors: Sign this to demand the accurate, high-visibility tools you need to protect your patients and shield your clinical practice from preventable legal crises.
Please sign and share this petition to close this invisible loophole once and for all. Your signature will force a tiny tech fix that will save thousands of lives and defend the healthcare workers who treat us.
👉 Click "Sign" now to fix the software flaw and protect patient safety 🫁
The Decision Makers
Petition Updates
Share this petition
Petition created on 11 June 2026